















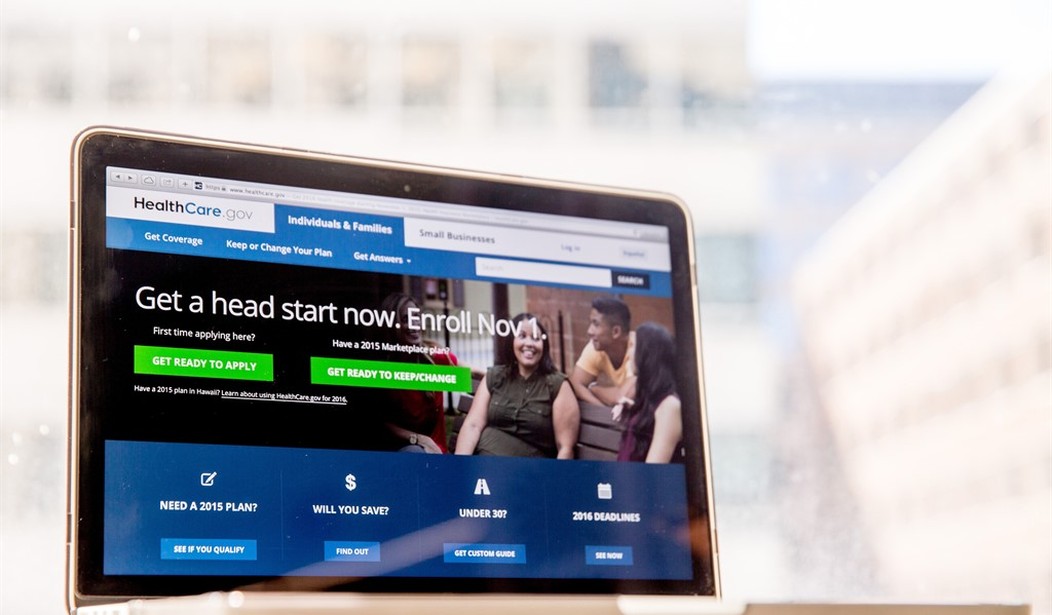
Many people believe Obamacare was designed to fail; intended as a steppingstone (or a speed bump) on the path to socialized medicine. One conspiracy theory posits that Obamacare proponents knew the exchanges would inevitably implode. Yet plotters figured after experiencing a decade of Obamacare’s painful dysfunction, the public would throw up its hands and accept a taxpayer-funded, socialized public plan option -- a Medicaid-For-All. In hindsight, that view was rather naïve. Obamacare is socialized medicine, just by another means.
Consider this: have you ever wondered why the government even cares whether you have health insurance? The Affordable Care Act (ACA) was supposedly designed to make health coverage affordable for millions of individuals who otherwise could not afford it. Moreover, the ACA was designed to make medical care “affordable” for many individuals by foisting the costs on others. Indeed, Obamacare was premised on the idea of forcing most people to pay for benefits far greater than their medical need to help subsidize others who may want medical care they cannot afford.
Health insurance and medical care are services that not everyone has the same demand for. Even controlling for health status, different people will want to see a doctor and pursue medical interventions at different rates. Just recently, a New York Times column discussed the problem with “one-size-fits-all health insurance” for people whose preferences and medical needs differ. Yet the Affordable Care Act purposely makes it difficult to economize on health coverage. The ACA does not allow individuals to take out a $25,000 deductible to lower premiums. Nor does it allow individuals to forgo medical benefits above, say, $500,000, even though $50,000 would be enough to finance care for about 99 percent of the population. For that matter, I know of no health insurance plans that will only cover medical care received in foreign countries.
The ACA was conceived from the idea that income and lifestyle should not limit access to medical care. Thus, requiring everyone to have comprehensive health insurance was a way to inject more resources into our health care system, which is not allowed to turn away money-losing customers or charge them more for their moral failings. Isn’t that the very definition of socialized medicine?

For example, a person who has led a healthy lifestyle does not qualify for a premium discounted lower than a similar-aged person whose lifestyle and health status is a hot mess. Someone who does not abuse IV drugs cannot agree to forgo high-priced treatments for hepatitis or opioid addiction. Let’s say you are a Christian or a Mormon, whose religious beliefs precludes alcohol, tobacco and other addictive substances. You cannot sign a waiver agreeing to forgo the right to chemical dependency treatments in return for lower premiums. After all, a party hearty kind of guy may need your drug treatment dollars.
And it doesn’t end there. A couple who has undergone a permanent contraceptive procedure cannot decline coverage for family planning or maternity benefits. Neither can you buy medical coverage that excludes maternity benefits just because you are male and incapable of having babies. Somebody else may want your baby dollars to have a kid on the cheap!
The “Affordable Care Act” is a misnomer. It did not make care affordable; quite the reverse for most people. The ACA made health coverage semi-affordable only for those newly-eligible for Medicaid and those earning up to 250 percent of the federal poverty level. The ACA took away the right of consumers to purchase the benefit package and type of coverage they prefer. It also took away the flexibility for insurers to experiment with varying plan designs. In the process, the ACA made health coverage decidedly unaffordable for millions of Americans who do not qualify for subsidies and have to purchase individual insurance on their own. ACA proponents’ attempt at socialized medicine through regulation turned out to be rather antisocial for most consumers. It’s time to repeal the costly regulations and replace them with something that allows coverage that is truly affordable (and flexible).
Devon M. Herrick, PhD is a health economist and senior fellow at the National Center for Policy Analysis.



Join the conversation as a VIP Member